CSDS team’s work was featured in The Australian Nursing & Midwifery Journal (ANMJ). They shared three articles in the October – December 2023 edition. In this blog post we are sharing the full article on the use of 3D animation to enhance midwifery education, written by Dr Kirsty McLeod, Dr Lisa Peberdy, Dr Mia McLanders, Ms Megan Barker and Dr Lauren Kearney.
BACKGROUND
Two-dimensional models (2D) (eg.pictures in textbooks) have traditionally been used to teach and guide complex clinical procedures. However, research suggests that introducing three dimensional (3D) models can reduce workload and improve performance in clinical skills training.
3D materials provide additional spatial information and have been found to assist in developing stronger mental models of internal anatomical structures and functions than 2D materials. 3D displays have also been found to support the development of minimally invasive surgical skills by helping to overcome visualisation and psychomotor challenges.
OVERVIEW OF EXISTING 3D ASSETS
Using a traditional apprenticeship-style approach to train high-risk and uncommon clinical procedures can jeopardise patient safety. Simulation-based training mitigates this risk by allowing clinicians to practice repeatedly in a safe space. However, accessing simulation-based training can be particularly difficult for rural and remote clinicians, and it often requires extensive time, resources, and financial commitments.
A market scan and informal training needs analysis revealed the limitations of current teaching aids in simulation-based shoulder dystocia and breech birth training – specifically, the limitations of representing complex manoeuvres in static illustrations and pictures.
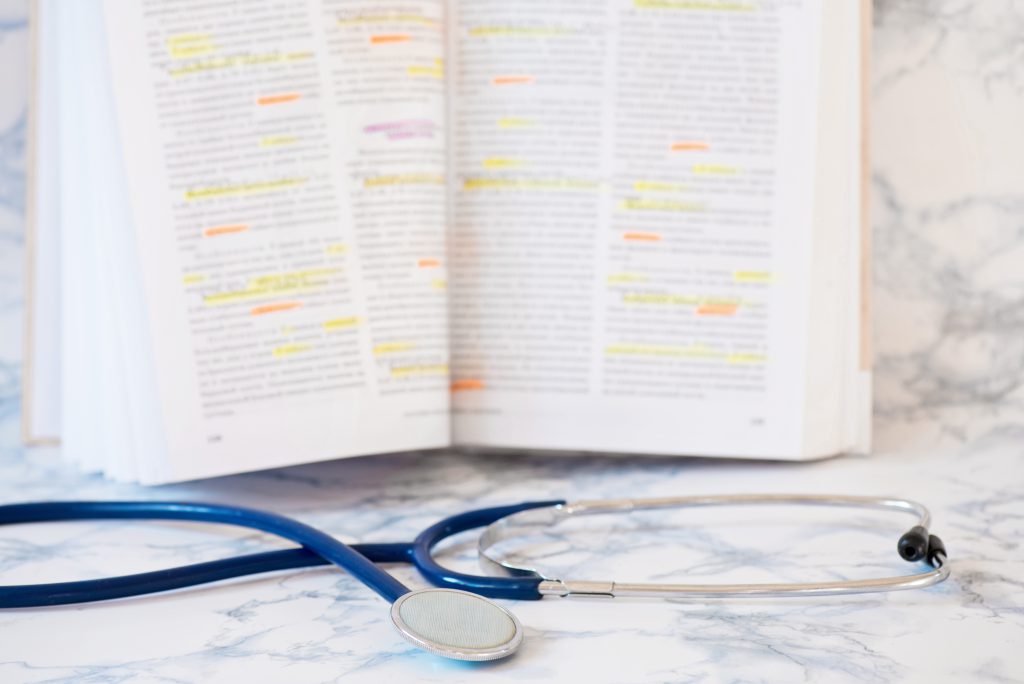
The Clinical Skills Development Service (CSDS) and Metro North Health Service, developed two online 3D animation tools to guide the training of complex manoeuvres for the management of shoulder dystocia and breech birth. The tools were developed to support knowledge acquisition and skill transfer to practice, and to aid learning by providing additional visuospatial cues. Multidisciplinary team was formed and comprised a clinical midwife consultant, obstetrician and gynaecology consultant, 3D developer, digital advisor, and evaluation officer. The 3D animation tools were sent to four midwifery subject-matter experts (SMEs) for review.
RESULTS
SMEs strongly agreed (75%) or agreed (25%) that the 3D animation was a valuable training tool for students learning how to manage shoulder dystocia. All SMEs strongly agreed (100%) that the 3D animation was a valuable training tool for students learning how to manage a breech birth. All SMEs agreed that the shoulder dystocia animation was clinically accurate. However, mixed results were found for the breech birth animation, with some disagreement from SMEs on the specifics of clinical accuracy.
CONCLUSION
3D animation can support the learning of complex psychomotor manoeuvres in midwifery education. However, introducing additional dimensions requires thorough investigation to ensure clinical accuracy from all viewing angles.
FUTURE PLANS
CSDS is revising the breech birth animation to ensure clinical accuracy, and future 3D training materials under consideration include the development of an online Perineal Assessment and Suturing Masterclass.
Do you have ideas or requests for improving healthcare through training, collaboration and innovation? Reach out to the CSDS team via the CSDS Idea and Request Form.